| • | Log-in to the practice, you should have ‘Admin” role to do this |
| • | Go to “Admin Page” |
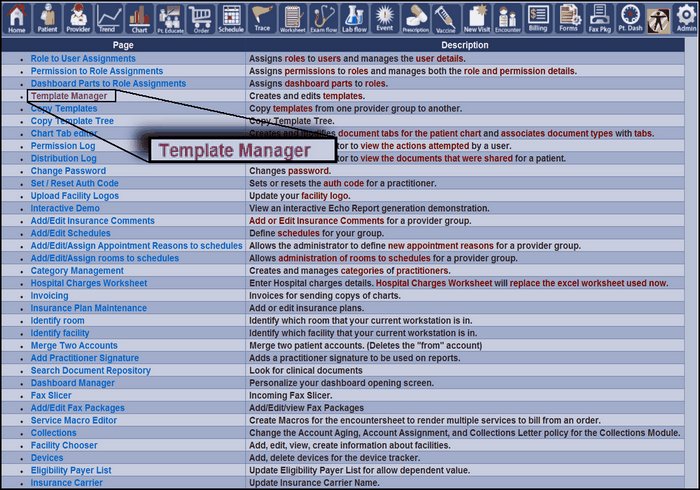
| • | Click on “Facility chooser” |
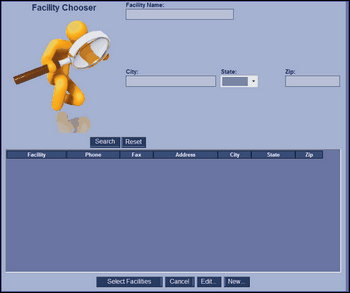
| • | Click on “new” |
| o | Information to have available |
| ▪ | Facility Name |
| ▪ | Contact First and Last name |
| ▪ | Facility Type |
| ▪ | Facility Association (relevant to the practice that this facility is associated with) |
| ▪ | Parent facility (if needed, if external) |
| ▪ | Specialty (required field) |
| ▪ | Mailing Address of facility (city, state, zip code) |
| ▪ | Phone numbers (primary, secondary, fax) |
| ▪ | EDI modem |
| ▪ |
| ▪ | Facility Logo Image file path |
| o | After entering all the above information, click submit to save |